Summary
Description
Chondroblastoma is a rare, benign tumor derived from chondroblasts. It is found in the epiphysis of long bones, usually of the lower extremity. The most common site is the distal femur followed by the proximal femur, proximal humerus and proximal tibia.
People and Age
The tumor has a preference for males over females and the mean age of presentation is approximately 20 years old.
Symptoms and Presentation
The tumor presents as a child, teenager or young adult with pain and swelling in a joint, usually the shoulder, knee, or hip. Occasionally the tumor can occur in the spine causing back pain.
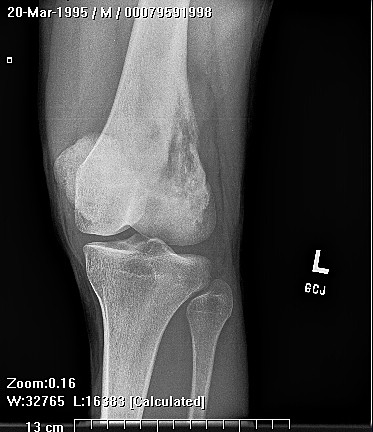
Brief description of the xray
In the xray, the tumor forms an expansile lesion in the epiphysis with calcifications
Brief desc of tx
Curettage is the treatment of choice for most of these tumors.
Tumor Name
Tumor Type
Benign or Malignant
Body region
Most Common Bones
Location in bone
Tumor behavior
Tumor density
Complete Information on this Tumor
Introduction and Definition
Chondroblastoma is a rare, benign tumor derived from chondroblasts. It is found in the epiphysis of long bones, usually of the lower extremity. The most common site is the distal femur followed by the proximal femur, proximal humerus and proximal tibia.
Incidence and Demographics
The tumor has a preference for males over females and the mean age of presentation is approximately 20 years old. The tumor may have behavior not normally associated with benign tumors including pulmonary metastases as well as local invasion of bone and soft tissue.
Symptoms and Presentation
Patients complain of aching pain in a joint. There is poor response to NSAID medication. Eventually a swelling or mass appears.
X-Ray Appearance and Advanced Imaging Findings
The diagnosis of chondroblastoma can usually be made by radiograph. when the age of the patient and location of the lesion are considered. The most common site for chondroblastoma is the epiphysis. The lesion is lytic with well defined margins and can be from 1-6cm in size. Scalloping or expansion of cortical bone may be present. Fine calcifications, either punctate or in rings, may be visible. Cysts are present about 20% of the time and both MRI and CT can define the fluid levels. CT is also useful for defining the relationship of the tumor to the joint, integrity of the cortex, and intralesional calcifications.
Differential Diagnosis
The differential diagnosis includes enchondroma, central chondrosarcoma and aneurysmal bone cyst.
Preferred Biopsy Technique for this Tumor
Incisional, may be combined with excision in selected cases
Histopathology findings
On gross examination, a chondroblastoma has a lobulated, round form and is made up of friable, soft, grayish pink tissue that may be gritty. If present, the cystic fluid is rust or straw-colored. Chondroblastoma is made up of uniform, polygonal cells that are closely packed. These primitive cells are derived from the epiphyseal cartilage plate and have abundant cytoplasm. These cells have oval shaped nuclei with a prominent groove which has been likened to a coffee bean. There is little mitotic activity. A scant chondroid matrix may be superimposed by a pericellular deposit of calcification that appears like "chicken-wire". The rapid proliferation of immature chondrocytes does not create lacunae or formal cartilage matrix. Giant cells are often present.
Treatment Options for this Tumor
Treatment of chondroblastoma is biopsy and curettage with possible use of adjuvant liquid nitrogen or phenol, or a mechanical burr. Due to the risk of recurrence and associated functional loss, the initial curettage should be as meticulous as necessary to ensure complete removal of the lesion. The surgical approach chosen should allow complete access to the lesion. Minimally invasive techniques that provide restricted access to the lesion should be avoided. It may be necessary to reconstruct articular surfaces due to subchondral erosion. Any joint invasion is usually secondary to previous instrumentation. All pulmonary nodules should be excised.
Preferred Margin for this Tumor
Intralesional
Outcomes of Treatment and Prognosis
Functional outcomes of surgical treatment of chondroblastoma are generally good, provided the tumor is not discovered very late and that the tumor does not recur. For lesions located in the proximal part of the femur and in the foot and ankle, recurrence is common, and outcomes are generally worse than in other locations in the skeleton. The risk of recurrence appears to be highest for lesions located only in the epiphysis, as opposed to lesions in the apophysis or those that extend into the metaphysis or diaphysis. Recurrence is not definitely related to patient age, sex or demographic data, but it is generally held that patients with open physes are at increased risk. Recurrent lesions should be treated with repeat curettage. If a recurrent lesion is very destructive or located in a readily reconstructable location, marginal resection with structural allograft or autograft reconstruction is preferable. Recurrence and severe destruction of bone integrity in the foot and ankle may necessitate ankle arthrodesis or en-bloc resection with associated functional loss. Patients with recurrent lesions should have follow-up CT scans of the chest to detect pulmonary nodules. Pulmonary nodules should be excised.
Special and Unusual Features
This is one of a very few lesions that occur primarily in the epiphysis. Others include clear cell chondrosarcoma and osteomyelitis. In addition, rare (v. rare) cases of metastasis to the lings have been reported. Usually the lesions in the lung may be observed, or treated with thoracoscopic assisted resection. Pheumothorax has been reported, inone case bilateral.
Suggested Reading and Reference
Bulloughs, Peter, Orthopaedic Pathology (third edition), Times Mirror International Publishers Limited, London, 1997.
Huvos, Andrew, Bone Tumors: Diagnosis, Treatment and Prognosis, W.B. Saunders, Co., 1991.
Huvos, Andrew, Bone Tumors: Diagnosis, Treatment and Prognosis, W.B. Saunders, Co., 1991.