Summary
Description
About 12% of all chondroblastomas occur in the bones of the foot.
People and Age
The average age at presentation around 25 years, significantly older than the average age in other parts of the skeleton.
Symptoms and Presentation
Patients complaint of pain and swelling or a mass near the joint. The pain can be severe. The nearby joint may be locally inflamed.
Brief description of the xray
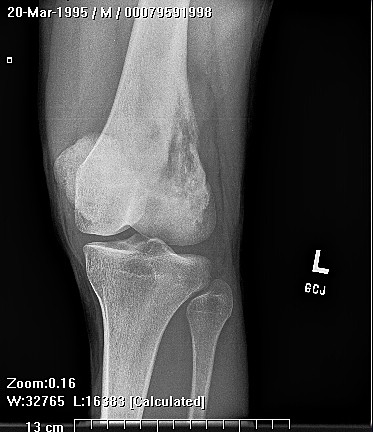
Radiographically, the lesion is located in the exclusively in the epiphysisis, although in the small bones of the foot the location of the epiphysis may not be obvious.
Brief desc of tx
Treatment of the primary lesion consists of complete curettage and bone grafting.
Tumor Name
Tumor Type
Benign or Malignant
Body region
Location in bone
Tumor behavior
Tumor density
Complete Information on this Tumor
Introduction and Definition
About 12% of all chondroblastomas occur in the bones of the foot. Chondroblastoma in the foot most commonly occurs in subchondral areas of the talus and calcaneus as well as the calcaneal apophysis. Chondroblastoma can behave aggressively and invade soft tissue. Benign pulmonary metastases have been observed.
Incidence and Demographics
Males are affected 6 times as commonly as females. The average age at presentation around 25 years, significantly older than the average age in other parts of the skeleton.
Symptoms and Presentation
Patients complaint of pain and swelling or a mass near the joint. The pain can be severe. The nearby joint may be locally inflamed.
X-Ray Appearance and Advanced Imaging Findings
Radiographically, the lesion is located in the exclusively in the epiphysisis, although in the small bones of the foot the location of the epiphysis may not be obvious. The lesions appear well-defined, expansile, and lucent, and there may be stippled calcification or there may be no matrix mineralization. The tumor is adjacent to an articular surface or an apophysis. There is a lobular appearance.
CT scan is useful for defining the relationship of the tumor to the joint, the integrity of the underlying bone, and to identify intralesional calcifications.
MRI scans show the very high signal intensity on T2 weighted scans that is characteristic of cartilage lesions.
Bone scan shows avid tracer uptake in the lesion.
CT scan is useful for defining the relationship of the tumor to the joint, the integrity of the underlying bone, and to identify intralesional calcifications.
MRI scans show the very high signal intensity on T2 weighted scans that is characteristic of cartilage lesions.
Bone scan shows avid tracer uptake in the lesion.
Treatment Options for this Tumor
Treatment of the primary lesion consists of complete curettage and bone grafting. Extending the zone of the curettage by removing two or 3 additional millimeters of bone using a mechanical bur, or by using phenol or liquid nitrogen placed in the tumor cavity have been proposed as in method to reduce the risk of local recurrence.
Outcomes of Treatment and Prognosis
In chondromblastoma of the foot and ankle, recurrence is common, and outcomes are generally worse than in other locations in the skeleton. The risk of recurrence appears to be highest for lesions located only in the epiphysis, as opposed to lesions in the apophysis or those that extend into the metaphysis or diaphysis. Recurrence is not definitely related to patient age, sex or demographic data. Recurrent lesions should be treated with repeat curettage. If a recurrent lesion is located in a readily reconstructable location, marginal resection with structural allograft or autograft reconstruction is preferable. Recurrence and severe destruction of bone integrity may necessitate ankle arthrodesis or en-bloc resection with associated functional loss. Patients with recurrent lesions should have follow-up CT scans of the chest to detect pulmonary nodules. Pulmonary nodules should be excised.
Suggested Reading and Reference
Fink BR, Temple HT, Chiricosta FM, Mizel MS, Murphey MD. Foot Ankle Int. 1997
Apr;18(4):236-42. Chondroblastoma of the foot.
Apr;18(4):236-42. Chondroblastoma of the foot.