Summary
Description
This rare benign tumor has a striking predilection for the bones of the tibia and the foot.
People and Age
Most patients are younger than 30.
Symptoms and Presentation
Patients present with pain and a slow growing mass.
Brief description of the xray
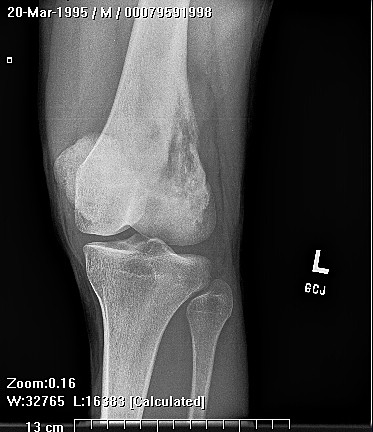
Radiological findings demonstrate an eccentrically placed Iytic lesion with well defined margins in the metaphysis of the lower extremity.
Brief desc of tx
Marginal or wide excision and substitution of the involved bone with a structural bone graft is usually curative.
Tumor Name
Tumor Type
Benign or Malignant
Body region
Most Common Bones
Location in bone
Position within the bone
Complete Information on this Tumor
Introduction and Definition
This rare benign tumor has a striking predilection for the bones of the tibia and the foot. About one quarter of all of these tumors involve the foot, with the metatarsals the most common location.
Incidence and Demographics
Most patients are younger than 30. It is more common in males, typically in the second or third decade of life.
Symptoms and Presentation
Patients present with pain and a slow growing mass.
X-Ray Appearance and Advanced Imaging Findings
Radiological findings demonstrate an eccentrically placed Iytic lesion with well defined margins in the metaphysis of the lower extremity. The lesion usually has a sclerotic margin of bone and a lobulated contour. Ridges and grooves that appear in the margins secondary to scalloping falsely appear to be trabeculae.
CT helps define cortical integrity and confirms that there is no mineralization of the matrix, unlike other cartilage tumors. CMF has the same appearance on MRI as other cartilage tumors which is decreased signal on T 1 weighted images and increased signal on T2 weighted images. MRI is helpful in preoperative planning and staging.
CMF resembles fibrocartilage grossly. It has a sharp border often with an outer surface of thin bone or periosteum. The glistening grayish white lesion is firm and lobulated. It may also have small cystic foci or areas of hemorrhage.
CT helps define cortical integrity and confirms that there is no mineralization of the matrix, unlike other cartilage tumors. CMF has the same appearance on MRI as other cartilage tumors which is decreased signal on T 1 weighted images and increased signal on T2 weighted images. MRI is helpful in preoperative planning and staging.
CMF resembles fibrocartilage grossly. It has a sharp border often with an outer surface of thin bone or periosteum. The glistening grayish white lesion is firm and lobulated. It may also have small cystic foci or areas of hemorrhage.
Differential Diagnosis
The radiologic differential diagnosis includes giant cell tumor, aneurysmal bone cyst, juxtacortical chondroma, unicameral bone cyst, chondroblastoma and fibrous dysplasia
Preferred Biopsy Technique for this Tumor
Careful biopsy and evaluation by an experienced pathologist are necessary to distinguish this tumor from similar aggressive or malignant lesions. Curettage may be adequate, but may result in local recurrence in as many as a quarter of patients.
Histopathology findings
Histologically, CMF appears very similar to chondrosarcoma. They are so close in histology that often radiology helps to make the final diagnosis. The predominant features of CMF are the zonal architecture and lobular pattern. Nodules of cartilage are found in between fibromyxoid areas. In some fields the loose myxoid dominates and in other the dense chondroid dominates. The chondrocytes are plump to spindly in shape and have indistinct cell borders in sparsely cellular lobules of myxoid or chondroid matrix. There are also more cellular zones of the tumor with some giant cells at the edges. The sharp borders of each lobule and the lesion itself help to differentiate it from chondrosarcoma.
Treatment Options for this Tumor
Marginal or wide excision and substitution of the involved bone with a structural bone graft is usually curative.
Outcomes of Treatment and Prognosis
Unlike giant cell tumor, this tumor has a propensity to recur due to seeding of the soft tissues during curettage. Local recurrence can be treated with meticulous repeat curettage and excision of the entire soft tissue mass. Marginal or wide excision and substitution of the involved bone with a structural bone graft is usually curative.