Summary
Description
Chondrosarcoma is a malignant mesenchymal tumor that produces cartilage matrix. There are several subtypes of chondrosarcoma, which vary in terms of location, appearance, treatment and prognosis.
People and Age
This tumor is more common in people over 60
Symptoms and Presentation
This tumor presents with pain and swelling in a bone
Brief description of the xray
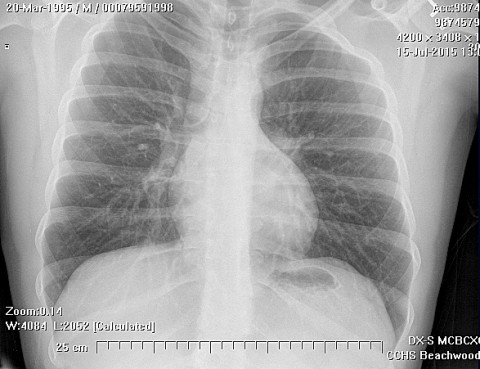
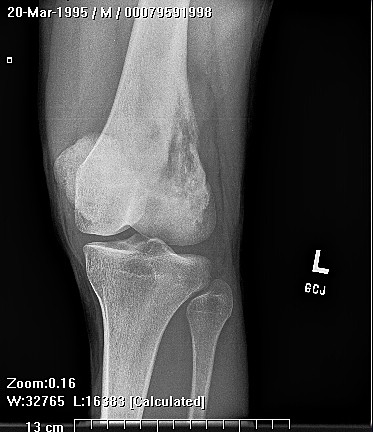
On plain radiographs, chondrosarcoma is a fusiform, lucent defect with scalloping of the inner cortex and periosteal reaction. Extension into the soft tissue may be present
Brief desc of tx
Complete surgical removal with a wide margin is the cornerstone of treatment
Complete Information on this Tumor
Introduction and Definition
Chondrosarcoma is a malignant tumor that produces cartilage matrix. Primary chondrosarcoma is very uncommon, arises centrally in the bone, and is found in children. Secondary chondrosarcoma arises from benign cartilage defects such as osteochondroma or enchondroma. Chondrosarcoma can also be classified as intramedullary, which generally arise from enchondromas, and surface which arise from osteochondromas.
Incidence and Demographics
Chondrosarcoma most commonly in adults aged 30 to 70 years, with the peak age of incidents being sometime around 40 to 60. Chondrosarcoma has a male to female ratio of 1.5 to 1. It is most common in the femur, humerus, ribs and on the surface of the pelvis. Patients with Ollier's disease (multiple enchondromatosis) or Maffucci's syndrome (multiple enchondromas and hemangiomas) are at much higher risk of chondrosarcoma than the normal population and often present in the third and fourth decade.
Symptoms and Presentation
The presentation of chondrosarcoma depends on the grade of the tumor. A high-grade, fast growing tumor can present with excruciating pain. A low grade, more indolent tumor is more likely to present as an older patient complaining of hip pain and swelling. Pelvic tumors present with urinary frequency or obstruction or may masquerade as "groin muscle pulls".
X-Ray Appearance and Advanced Imaging Findings
On plain radiographs, chondrosarcoma is a fusiform, lucent defect with scalloping of the inner cortex and periosteal reaction. Extension into the soft tissue may be present as well as punctate or stippled calcification of the cartilage matrix. CT is helpful in defining the integrity of the cortex and distribution of calcification. MRI is invaluable in surgical planning as it demonstrates the intraosseus and soft tissue involvement of the tumor. MRI is also helpful in evaluating possible malignant degeneration of osteochondromas by allowing accurate measurements of the cartilage cap which should be less than 2 cm thick.
Differential Diagnosis
Osteosarcoma, benign cartilage lesions
Preferred Biopsy Technique for this Tumor
Incisional
Histopathology findings
On gross examination, chondrosarcoma is a grayish-white, lobulated mass. It may have focal calcification, mucoid I degeneration, or necrosis.Histologically, chondrosarcoma is differentiated from benign cartilage growths by enlarged plump nuclei, multiple cells per lacunae, binucleated cells, and hyperchromic nuclear pleomorphism. Chondrosarcoma is graded from 1 (low) to 3 (high). Low grade chondrosarcoma is very close in appearance to enchondromas and osteochondromas and has occasional binucleated cells. High grade chondrosarcomas have increased cellularity, atypia and mitoses. There is an inverse relationship between histologic grade and prognosis with higher grades having a worse prognosis and early metastases.
Treatment Options for this Tumor
Treatment of chondrosarcoma is wide surgical excision. Controversy exists and treatment is highly individualized, based on location, stage, subtype, and patient factors. Treatment choices are determined largely by geographic and institutional factors, rather than tumor characteristics. Chemotherapy and radiation treatments for central chondrosarcoma are not well supported by validated outcomes data. The role for chemotherapy or radiation is currently unknown. A recent publication (Leddy Cancer Treat Res. 2014;162:117-30) stated that surgery is the only treatment for chondrosarcoma. However, certain subtypes of chondrosarcoma may be responsive to chemotherapy. For nonmetastatic mesenchymal chondrosarcoma, chemotherapy as well as negative surgical margins have been shown to be associated with improved overall and event-free survival in some trials (Frezza, Eur J Cancer. 2015 Feb;51(3):374-81.). Biopsies must be planned with future tumor excision in mind.
Preferred Margin for this Tumor
wide
Outcomes of Treatment and Prognosis
Survival of chondrosarcoma is difficult to precisely define because of the large number of subtypes, varying histologic grades of the tumor, and a wide variety of treatments that are given depending on tumor extent that location. Patients with adequately resected low grade chondrosarcomas have an excellent survival rate. In general the survival of patients with high grade tumors varies depending on the location, subtype, effectiveness of surgical treatment, size and stage of the tumor.
Recent data from a relatively homogeneous group of patients with primary central chondrosarcoma who presented with localized disease are available. These data (Andreou 2011) focus only on primary central chondrosarcoma in 115 patients treated in a cancer center in Europe. Overall survival at five years was 72% and 69%. Event-free survival at five and 10 years was 57% and 53%.
One of the most striking findings in the (Andreou 2011) data concern the development of local recurrence and distant metastasis. The authors found that both local recurrence and distant metastasis lead to a significant decrease in overall survival regardless of tumor grade and regardless of localization. In this group of patients, long-term survival was only possible if the recurrence or metastasis was completely resected with wide margins.
In this recently published data (Andreou 2011), certain factors had positive or negative impact on survival. The AJCC stage did not correlate with oncological outcome in patients with tumors of the axial skeleton or pelvis. The authors suggest that a separate staging system for these tumors might be justified. Chondrosarcoma located in the extremity had statistically better survival than chondrosarcoma located in the axial skeleton. There was no difference in survival between males and females. The age of the patient at diagnosis had a statistically significant impact on survival. Patients under age 40 fared better than those older. Tumor volume was also statistically significant. Patients with tumors smaller than 100 cm³ had better overall and event free survival. Low-grade tumors had better survival than high-grade tumors. In this study, the quality of surgical margins did not affect survival, even when tumor grade and localization were taken into account. However, multiple other groups have reported that inadequate surgical margins were associated with poor prognosis. Controversy remains over this topic, and questions have arisen over the statistical methods used in the previous studies.
Special and Unusual Features
There are three additional types of chondrosarcoma. Mesenchymal chondrosarcoma is a rare variant with a bimorphic histologic picture of low grade cartilaginous cells and hypercellular small, uniform, and undifferentiated cells that resemble Ewing's sarcoma. Mesenchymal chondrosarcoma has a predilection for the spine, ribs and jaw and it presents in the third decade. It is more common in females and can grow exceptionally large. It is very likely to metastasize to lungs, Iymph nodes and other bones. Clear cell chondrosarcoma is a malignant cartilage tumor that may be the adult variant of chondroblastoma. It is a rare, low-grade tumor with an improved prognosis over other chondrosarcomas. Likechondroblastoma, it is found in the epiphysis of the femur and humerus. Histologically, soft tissue invasion is rare. Clear cell chondrosarcoma has clear cells with vacuolated cytoplasm. The cartilage matrix has significantly calcified trabeculae and giant cells. Dedifferentiated chondrosarcoma is the most malignant form of chondrosarcoma. This tumor is a mix of low grade chondrosarcoma and high grade spindle cell sarcoma where the spindle cells are no longer identifiable as having a cartilage origin. The dedifferentiated portion of the lesion may have histological features of malignant fibrous histiocytoma, osteosarcoma, or undifferentiated sarcoma. This biphasic quality is evident on x-ray with areas of endosteal scalloping and cortical thickening are contrasted with areas of cortical destruction and soft tissue invasion. Dedifferentiated chondrosarcoma has a 5 year survival of 10%.
Suggested Reading and Reference
Andreou, et al, Acta, 2011 82 (6) 749 - 755