Summary
Description
Hemangiomas are benign bone lesions characterized by vascular spaces lined with endothelial cells. Approximately 50% of osseous hemangiomas are found in the vertebral bodies (thoracic especially) and 20% are located in the calvarium. The remaining lesions are found in the tibia, femur and humerus.
People and Age
Peak incidence occurs in the 50s.
Symptoms and Presentation
Hemangiomas are largely asymptomatic, usually found incidentally.
Brief description of the xray
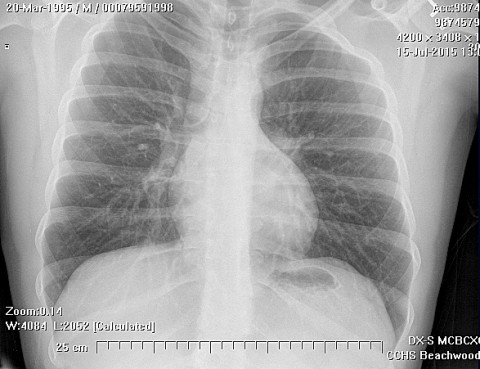
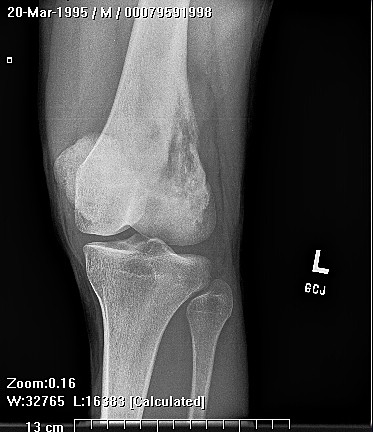
Appearance on X-ray is dependent on location. The lesions are often poorly defined, appearing as a somewhat localized area of abundant, dilated vessels, some of which may be on the surface of the bone, within the cortex of the bone, or extend into the medullary cavity.
Complete Information on this Tumor
Introduction and Definition
Hemangiomas are benign bone lesions characterized by vascular spaces lined with endothelial cells. Debate continues as to the pathogenesis and proper classification of these lesions.
Incidence and Demographics
Hemangiomas are largely asymptomatic, and thus most are never discovered, leading some to describe these lesions as "rare". In actuality, hemangiomas are common lesions with approximately 10% of autopsy cases having vertebral hemangiomas in one study. The peak incidence is in the fifth decade.
Approximately 50% of osseous hemangiomas are found in the vertebral bodies (thoracic especially) and 20% are located in the calvarium. The remaining lesions are found in the tibia, femur and humerus.
Symptoms and Presentation
Hemangiomas are usually asymptomatic lesions discovered on x-ray or autopsy. Vertebral hemangiomas can cause neurological symptoms if they extend into the epidural space. Symptoms may vary with other factors that cause vascular distension or reactivity, such as dependency, activity, pregnancy and menstruation.
X-Ray Appearance and Advanced Imaging Findings
The radiological appearance can be quite striking and depends on the location of the lesion. In the long bones the lesions are usually located in the metaphysis or diaphysis. The lesions have a propensity to extend from the bone into the surrounding soft tissues, or vice versa. The lesions are often poorly defined, appearing as a somewhat localized area of abundant, dilated vessels, some of which may be on the surface of the bone, within the cortex of the bone, or extend into the medullary cavity. Normally there are multiple, small, somewhat irregular lytic areas surrounded by variable areas of scelrosis. (see images)
Vertebral lesions have thickened vertebral trabeculae secondary to erosion of the horizontal trabeculae which gives a "corduroy" appearance on plain film. On axial CT scan, vertebral body lesions have a "polka dot" pattern as the vessels are seen in cross section. Calvarial lesions are lytic and resemble radiating wheel spokes. Hemangiomas in the metaphysis or epiphysis of long bones are lytic lesions that give a spiculated pattern known as "Irish lace". T1 weighted MRI scans vary from low to high intensity depending on the amount of adipose tissue present. T2 weighted MRI scans demonstrate lesions with high intensity due to the vascularity.
MRI Findings
T1 weighted MRI scans vary from low to high intensity depending on the amount of adipose tissue present. T2 weighted MRI scans demonstrate lesions with high intensity due to the vascularity.
CT Findings
On axial CT scan, vertebral body lesions have a "polka dot" pattern as the vessels are seen in cross section.
Differential Diagnosis
This tumor has a unique appearance on plain x-rays that is diagnostic when present. Other lesions that may have a similar periods include infection, lymphangiomatosis.
Histopathology findings
On gross examination, hemangiomas look like a disorganized collection of veins or vascular spaces. Grossly there are cystic, dark red cavities. The lytic areas are sharply defined and there is trabecular thickening.
Under the microscope, there are four types of hemangiomas: capillary, cavernous, arteriovenous and venous. Capillary and cavernous lesions are the most common in bone. Capillary hemangiomas contain capillary size vessels lined by flattened endothelial cells. Cavernous hemangiomas are often found in the calvaria and contain large dilated vessels with flattened endothelium. Arteriovenous hemangiomas are remnants of fetal capillary beds and venous hemangiomas contain small thick-walled venous vessels. Non-vascular components of hemangiomas include fat, smooth muscle, fibrous tissue, bone, hemosiderin and thrombus.
Treatment Options for this Tumor
Treatment of hemangioma is unnecessary unless the lesion is symptomatic. Minor discomfort may be treated with compression of he lesion using vascular stockings, ace wraps, or compression tights or shorts. Surgeons should avoid treatment of minorly symptomatic lesions. Painful intraosseous lesions without cord compression may be treated with balloon kyphoplasty, vertebroplasty or transarterial embolization. In the spine, hemangiomas may compress the cord without causing instability or deformity, and these are best treated with conservative surgical removal. More aggressive lesions are treated with embolization followed by complete intralesional spondylectomy.
Lesions in the calvarium should be resected with a thin margin of normal bone.
Painful long bone lesions may also be treated with direct sclerotherapy, intralesional excision or or transarterial embolization. Large lesions in long bones should be excised and packed with bone graft if appropriate. There have been sporadic reports of serious bleeding from these lesions during surgery, and caution is advised with large or deeply placed lesions.
Suggested Reading and Reference
Conway, WF and CW Hayes, Miscellaneous Lesions of Bone, Radiologic Clinics of North America, 31(2):339-357, March, 1993.
Murphey, MD et al., Musculoskeletal Angiomatous Lesions: Radiologic-Pathologic Correlation, Radiographics, 15(4):892-917, July, 1995.
Bullough, Peter. Orthopedic Patholovv (third edition), Times Mirror
International Publishers Limited, London, 1997.
Huvos, Andrew, Bone Tumors:Diagnosis. Treatment and Prognosis, W.B. Saunders, Co., 1991.