Summary
Description
Synovial chondromatosis is the rare and benign metaplasia of the synovial membrane resulting in the formation of multiple intra-articular cartilaginous bodies. Synovial chondromatosis is known by several other names including articular chondrosis and synovial chondrosis. This self-limited and non-aggressive condition occurs most commonly in the knee followed by the hip, shoulder and elbow.
People and Age
It presents during the third to fifth decade twice as often in men than women and does not occur in children.
Symptoms and Presentation
Synovial chondromatosis presents as the gradual onset of monoarticular pain and stiffness. If allowed to continue, the slow, progressive symptoms can result in decreased range of motion, effusions, crepitation and eventual locking of the joint. This condition has also been described in the synovium, soft tissue and bursae. Secondary synovial chondromatosis may be present after long standing osteoarthritis.
Brief description of the xray
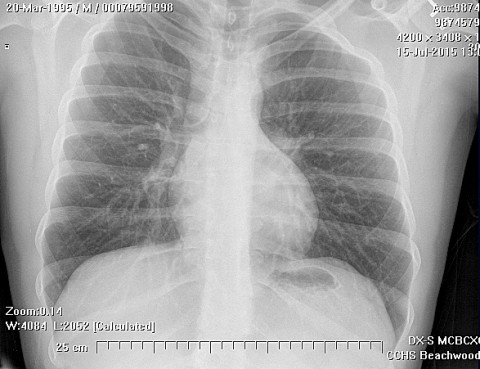
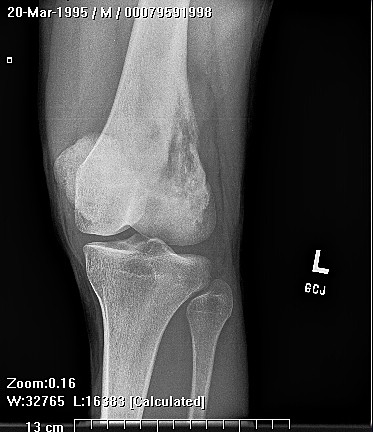
On a simple X-ray synovial chondromatosis is usually that of radiopaque round or oval loose bodies within the joint. Other radiologic signs include effusion, degenerative arthrosis, osteophytes and subchondral sclerosis.
Complete Information on this Tumor
Introduction and Definition
Synovial chondromatosis is the rare and benign metaplasia of the synovial membrane resulting in the formation of multiple intra-articular cartilaginous bodies. Synovial chondromatosis is known by several other names including articular chondrosis and synovial chondrosis. This self-limited and non-aggressive condition occurs most commonly in the knee followed by the hip, shoulder and elbow.
Incidence and Demographics
It presents during the third to fifth decade twice as often in men than women and does not occur in children.
Symptoms and Presentation
Synovial chondromatosis presents as the gradual onset of monoarticular pain and stiffness. If allowed to continue, the slow, progressive symptoms can result in decreased range of motion, effusions, crepitation and eventual locking of the joint. This condition has also been described in the synovium, soft tissue and bursae. Secondary synovial chondromatosis may be present after long standing osteoarthritis.
There are several possible etiologies for synovial chondromatosis. Trauma is supported by the fact that the process occurs primarily in weight bearing and dominant upper extremity joints. Infection is another possible culprit. Another theory postulates that cartilage shed into the joint is taken up by the synovium.
X-Ray Appearance and Advanced Imaging Findings
The radiologic appearance of synovial chondromatosis is usually that of radiopaque round or oval loose bodies within the joint. Other radiologic signs include effusion, degenerative arthrosis, osteophytes and subchondral sclerosis. CT scan is useful for viewing loose bodies that may not have calcified and are not visible on plain x-ray. MRI demonstrates multiple small filling defects and offers no real advantage over CT scan. Bone scan has increased uptake around calcified loose bodies. Contrast arthography is
another option for delineating the presence of loose bodies. The differential diagnosis of synovial chondromatosis includes septic arthritis, PVNS, rheumatoid arthritis, osteoarthritis and synovial sarcoma.
Differential Diagnosis
On gross examination, there is diffuse or focal involvement of the synovium with multiple nodules. The nodules are white-gray, translucent hyaline cartilage and range in size from lmm to 3cm. Nodules are often concentrated near the synovial cartilage junction and eventually break free from the
Histopathology findings
Under the microscope, synovial chondromatosis appears as focal islands of disorganized hyaline cartilage metaplasia in synovium. This condition has aggressive cytologic features including enlarged chondrocytes, hypercellularity and pleomorphic nuclei but is a benign, self limited condition.
Treatment Options for this Tumor
Treatment of synovial chondromatosis is controversial. Options include arthroscopic synovectomy, open synovectomy and loose body removal.
Special and Unusual Features
Milgram defined three phases of synovial chondromatosis: active intrasynovial disease (metaplasia without loose bodies), transitional lesions (metaplasia with loose bodies) and quiescent intrasynovial disease (loose bodies without metaplasia). Nodules may calcify or ossify. In rare cases, sarcomatous degeneration has occurred.
Suggested Reading and Reference
Milgram, JW, Synovial osteochondromatosis: A Histopathological Study of Thirty Cases, Journal of Bone and Joint Surgery. 59A:792-801, 1977.
Bullough, Peter, Orthopaedic Pathologv (third edition), Times Mirror International Publishers Limited, London, 1997.
Huvos, Andrew. Bone Tumors: Diagnosis. Treatment and Prognosis, W.B. Saunders, Col, 1991.
Crotty, JM et al., Synovial Osteochondromatosis, Radiologic Clinics of North America, 34(2):327-341, March, 1996.
Coles MH and HH Tara, Synovial Chondromatosis:A Case Study and Brief Review. American Journal of Orthopedics, 26(1):37-40, Jan, 1997.
Gilbert SR and PF Lachiewicz, Primary Synovial Osteochordromatosis of the Hip. Report of Two Cases with long-term Follow-Up After Synovectomy and a Review of the Literature, American Journal of Orthopedics. 26(8):555-60, August, 1997.