Summary
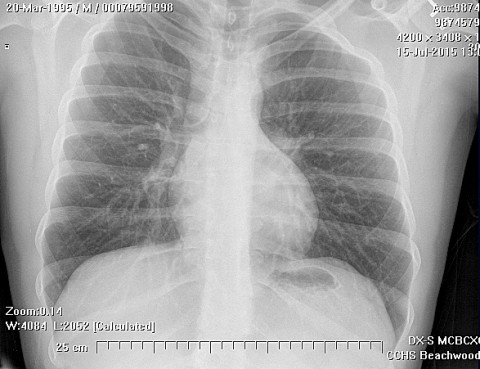
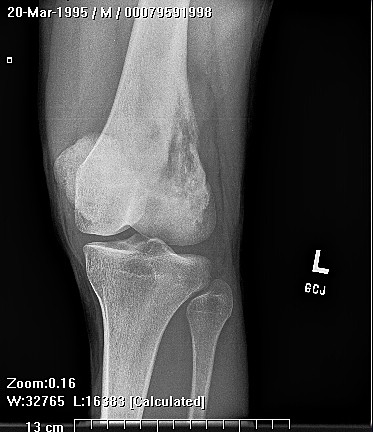
This rare form of chondrosarcoma is a deadly high grade sarcoma consisting of primitive mesenchymal cells and islands of cartilage which occurs most often in the femur, ribs, jaw, skull, and spine, and may occur in any bone.
Complete Information on this Tumor
This rare form of chondrosarcoma is a tumor of undifferentiated mesenchymal cells mixed with areas of cartilage. It occurs most often in the femur, ribs, jaw, skull, and spine, and may occur in any bone. This form of chondrosarcoma is usually high grade, and the tumor is characterized by more frequent local recurrence and metastasis and a relatively poor prognosis. The xray features are not diagnostic but the histopathology is constant.
Patients present with local pain and a mass. Headache occurs in the skull lesions. Base of skull lesions present with brainstem symptoms, and cranial nerve dysfunction.
Mesenchymal chondrosarcoma. An analysis of patients treated at a single institution.