A metastatic cancer in the foot may appear at first to be a common complaint, such as plantar fasciitis, metatarsalgia, or midfoot arthritis. This module contains everything you need to know to make a prompt and accurate diagnosis in these cases.
To avoid misdiagnosis, diagnostic delay, and errors in management, the foot and ankle specialist should be familiar with the basic facts about metastatic tumors in the foot. Due to the variety and scarcity of these tumors, the clinician cannot anticipate how the patient with this condition will present. The findings in these cases may at first point to a common foot ailment, but the presentation isn’t exactly as it should be. The clinician must stay vigilant and maintain a healthy index of suspicion, so as to avoid missing the subtle anomalies these cases present. Keen observation, a thorough medical history, and a careful examination should result in few or none of these tumors escaping prompt diagnosis. Once the alert clinician has noticed that small anomaly, the appropriate diagnostic approach is usually straightforward.
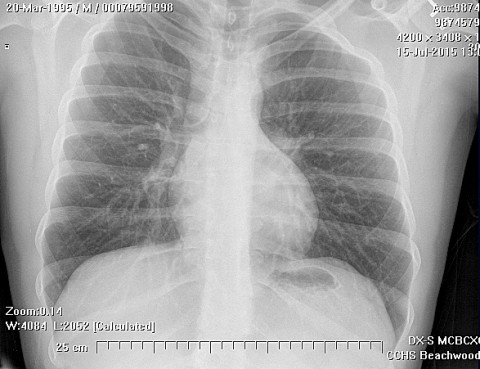
Once the possibility of a metastatic cancer in the foot has been considered, management should consist of two high quality orthogonal radiographs of the area of interest. If a definite bone lesion is seen on the plain radiographs, a computed tomography scan and a magnetic resonance imaging scan should be obtained. The medical history should be reviewed or repeated with an emphasis on family and personal cancer history and the status of routine screening studies, such as mammography, colonoscopy, pap smear, stool guiaic, and the like. In many instances, this information will lead to the discovery of a likely primary source of the bone lesion.
Metastases distal to the knee are unusual, and metastases to the bones of the foot are even more rare.(1) Metastases to bone develop in 30 % of all patients with cancer, with only 0.007 to 0.3 % having acrometastases.(3) Libson et al 1987 in their report, found that the most common sources were the colorectal, renal and lung carcinomas (50%), with the bladder, uterus and breast responsible for 25% of metastases to the foot.(4) Zindrick et al (1982), found the main sources of metastases to the bones of the feet to be the genitourinary tract and colon.(1,5) The average interval from diagnosis of primary tumor until bone metastasis is reported to be approximately 3 years. (6) Malignant tumors can metastasize to the soft tissues as well as to the bones of the feet (ref.). Metastases from renal cell carcinoma usually affect bones, less so the soft tissue, and rarely both bones and soft tissue.(7) Sarcomas have also been reported to metastasize to the foot. (3, 8)
One study found that out of tumors of the foot, 14.7% were metastatic, and the talus was the most commonly affected, then the calcaneus.(9) They also found (past tense) the gastrointestinal tract to be the commonest source. The tarsal bones are (present tense) involved in 50% of the cases, the metatarsals in 23%, whereas the phalanges account for only 17% of the reported cases.(5) In the series reported by Healey et al, 1982, the calcaneus was most commonly affected, while the talus was not affected at all.(3) Zindrick et al mentioned that the calcaneus was concomitantly affected in 45% of tarsal metastases.(1,5) Metastases to the distal phalanges of the toes are rare,(5) accounting for less than 0.05% of all bone metastases.(4) Rarely, widespread involvement of multiple contiguous foot bones may occur.(1)
Healey et al, Perdona et al, and Amiot et al have stated that acrometastases develop as part of widespread tumor spread (3,7,10) and as a pre-terminal event.(3) Such metastases occur late in the disease and indicate a poor prognosis.(7,10) Failure to recognize these lesions often leads to delay in diagnosis, or offering inappropriate treatment.(3) Presentation of metastases to the foot is very variable and will usually present late to the tumor surgeon. Such variability and late presentation is mostly seen when metastases affect the toes, where clinically these lesions may be mistaken for felon, whitlow, acute paronychia, gout, rheumatoid arthritis, osteomyelitis, infected hematoma or even an ingrown toe nail.(10) On the contrary, Ozdemir et al 1997 mention that due to the foot's compact structure and weight-bearing functions, both bone and soft tissue tumors are noticed early (11). Common complaints include foot pain, localized or diffuse swelling which is progressively enlarging, subungual lesion or an ulcerated discharging lesion. Some patients even have pain before any radiographic changes can be detected.(12) Clinical features of metastasis to the phalanges includes redness, warmth, swelling, ulceration, or tenderness.(5) In a case report on metastatic renal cell carcinoma to the big toe, this presented as an enlarging subungual nodule that displaced the nail.(5) Yadav et al 2004 reported a large tender non-pulsatile swelling of the midfoot.(13) Foot pain was the main presenting feature in many reports (ref.), while an enlarging swelling was reported in renal cell carcinoma. Rarely, metastatic disease to the foot can present without pain and in an unusual location, as Ali et al 2003, have reported on painless gross swelling of the fourth toe.(8)
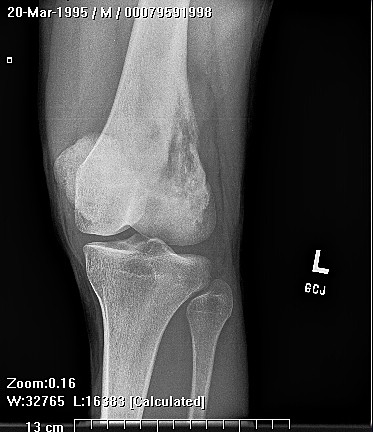
Radiologic signs on plain x-rays will vary depending on the type and aggressiveness of the tumor and the time elapsed until presentation. These include soft tissue swelling, moderate to marked bone destruction, and in some cases complete bone lysis.(5) Bone lysis is usually without any periosteal reaction.(1,14) When the distal phalanx of the big toe is the site of the lesion, the joint is rarely involved or crossed by the lesion(1) , and a thin margin of subchondral bone usually remains, even with extreme destruction.(1,5) The subchondral bone plate as well as the joint space are usually preserved.(5) The neoplasm may cause ballooning of the thinned cortical shell as it enlarges.(1) Cortical ballooning may be seen with metastases.(5) Metastases to the foot from prostatic carcinoma, although very rare, have a characteristic appearance where lesions are sclerotic with intact cortices, although one case of lytic metastasis has been reported.(15) If the tumor has broken through the cortex, there is a homogenous soft tissue involvement.(1) Yadav et al 2004 reported finding expansion and extensive destruction of the second metatarsal by a soft tissue mass that replaced the entire metatarsal.(13) Also, in rare cases, involvement may be so extensive such that destruction may involve the hindfoot and metatarsals.(16)
Even though distant metastases occur by vascular invasion, the exact mechanism of tumor spread to the distal parts of the extremities in still unclear.(10, 17) The dominant hand was found to be affected with metastases twice as common as the non-dominant hand, raising the possibility of increased blood supply as a cause for metastases.(3) Metastases from primary lung carcinoma can reach the systemic circulation when tumor cells erode the pulmonary capillaries in the lung, from where they can disseminate widely.(1) Another possible explanation is tumor cells drain via lymphatics then gain access to the venous system, from which they enter the systemic circulation and spread distally.(18) Batson has demonstrated how the valveless venous plexus in the paravertebral region communicates with the vessels of the lower extremities, hence venous flow from the pelvic veins could reach the vertebral venous system then to the vessels of the lower limbs.(19) (are you really proposing that Batson’s plexus reaches the foot?? did someone really state this) Since this valveless system communicates with the iliofemoral venous system, and since the incompetent iliofemoral system is unable to compensate for gravitational forces, this allows tumor emboli to reach the foot.(20) Using this explanation, it follows that tumors in subdiaphragmatic locations are more prone to metastasize to the lower extremities. The presence of red, active marrow has been shown to increase the likelihood of metastasis, possibly due to increased blood flow or a more favorable microenvironment.(21) The absence of red marrow in the bones of the feet could explain the rarity of metastases to the bones of the feet.(20,22, 23) A history of trauma, local temperature, hormonal influences, and local hemodynamics may also contribute to the development of these metastases.(5)
It is apparent from the review of literature that many cases present to the surgeon mimicking other benign processes, and thus a systematic workup for tumor metastasis is not done prior to surgery. Instead, the lesion is removed as part of an amputation process and sent for histopathology, to reveal the diagnosis of metastatic disease. The importance of a biopsy cannot be overemphasized. A biopsy should be obtained of any questionable lesion,(1) as a definite histopathologic diagnosis is required. The appropriate type is an incisional biopsy (11). Sebag-Montefiore et al 1997, stress the importance of a definitive diagnosis, based on a histologic confirmation, such that palliative radiotherapy may be given in tumors or antibiotics given in cases of infection.(24) Renal cell carcinoma acral lesions may also mimic other malignancies microscopically, especially adenocortical carcinoma, clear cell sarcoma and malignant melanoma, and this mandates the use of immunohistochemical stains. Any patient with a known history of metastatic carcinoma, presenting with evidence of bony destruction, should have a biopsy performed.(10) CT scan of the foot was done as part of the initial workup but the lesion appeared benign. (12) in one study, I have read the use of Tc scan of the foot, and in two separate studies, a CT of the foot was done.(Ramkumar)
Frequently, diagnosis is delayed or a misdiagnosis is made, especially when there is no history of primary disease or no complaints from a primary site of malignancy.(11, need references here) Diagnosis may be delayed from 1-3 months. In conditions when a painful swelling occurred suddenly and grew rapidly, and especially so when there was previous history of a known primary malignancy, diagnosis was made early, even if after the toe was amputated or lower leg amputation performed. In renal cell carcinoma, the behavior of a metastatic lesion is totally unpredictable, yet early diagnosis and treatment holds hopes for positively affecting patient survival.(7)
Kaplansky et al 2006, mentioned that when a metastasis is discovered, the patient has average survival of 3-9 months.(5) In the study by Hattrup et al, 1988, the patients had a mean survival of 12.3 months after detection of the metastasis. Also in that same study, patients treated surgically had mean survival of 16.5 months, while those treated by radiotherapy had 10.3 months only.(25) Other articles have documented longer patient survival, in some reaching 20 months after toe amputation.(16) Schwartz et al, support the idea that current advances in cancer therapy can prolong survival, thus timely diagnosis may be helpful. In the report by Cooper et al, the patient was disease free 5 years after successful treatment of her foot metastasis from a differentiated endometrioid carcinoma.(18)
Recent advances in cancer treatment are likely to lead to changing patterns of metastasis and acrometastasis. In colon cancer, the incidence bone metastasis appears to be increasing (reference here). However, widespread adoption of bishosphonate treatment for patients with advanced breast, prostate, and multiple melanoma cancers has lead to a significant decrease in their risk of skeletal metastasis.(reference here) Although the numbers are too small to analyze for statistical significance, it appears that the risk of acrometastasis from color cancer may be increasing at the present time, while the risk of acrometastasis from other tumors, such as breast and prostate cancer, may be decreasing.
References:
References:
1. Zindrick MR, Young MP, Daley RJ, Light TR. General orthopaedics, metastatic
tumors of the foot: case report and literature review. Clin Orthop Rel Res 1982;170:
219- 225.
2. Leeson MC, Makley JT, Carter JR. Metastatic skeletal disease distal to the elbow
and knee. Clin Orthop 1986; 206: 94- ??.
3. Healey JH, Turnbull ADM, Miedema B, Lane JM. Acrometastases. A Study of
Twenty Nine patients with Osseous Involvement of the Hands and Feet. J Bone
Joint Surg Am. 1986; 68: 743-746.
4. Libson E, Bloom R, Husband J, Stoker D. Metastatic tumors of bones of the hand
and foot: a comparative review and report of 43 additional cases. Skeletal Radiol
1987; 16: 387-392.
5. Kaplansky DB, Kademian ME, Vancourt RB. Metastatic Squamous Cell
Carcinoma resembling Cellulitis and Osteomyelitis of the Fifth Toe. J Foot Ankle
Surg. 2006; 45(3):182-184.
6. Sahinler I, Erkal H, Akyazici E, Atkovar G, Okkan S. Endometrial carcinoma and
an unusual presentation of bone metastasis: a case report. Gynecol Oncol 2001;82:
216-218.
7. Perdona S, Autorino R, Gallo L, De Sio M, Marra L, Claudio L, Caraco C, Franco
R, Fazzioli F, Gallo A. Renal Cell Carinoma with Solitary Toe Metastasis. Int J
Urol. 2005; 12: 401-404.
8. Ali ZA, Wimhurst JA, Ali AA, Tempest ME, Edwards DJ. Endometrial cancer
metastasis presenting as a grossly swollen toe. Int J Gynecol Cancer 2003; 13:
909-911.
9. Bakotic B, Huvos A. Tumors of the foot: a review of 150 cases. J Foot Ankle Surg.
2001; 405: 277-286.
10. Amiot RA, Wilson SE, Reznicek MJ, Webb BS. Endometrial Carcinoma
Metastasis to the Distal Phalanx of the Hallux: A Case Report. J Foot Ankle Surg.
2005; 44(6):462-465.
11. Ozdemir HM, Yildiz Y, Yilmaz C, Saglik Y. Tumors of the Foot and Ankle:
Analysis of 196 Cases. J Foot Ankle Surg. 1997; 36(6): 403-8.
12. Ramkumar U, Munshi NI, El-Jabbour JN. Occult Carcinoma of the Lung
Presenting as Pain in the Hallux: A case Report. J Foot Ankle Surg. 2005;
44(6):483-486.
13. Yadav R, Ansari MS, Dogra PN. Renal Cell Carcinoma Presenting as Solitary
Foot Metastasis. Int Urol Nephrol 2004; 36: 329-330.
14. Sundberg SB, Carlson WO, Johnson KA. Metastatic lesions of the foot and ankle.
Foot Ankle 1982; 3: 167-169.
15. Schwartz ED, Donahue FI, Bromson MS, Blaise JF. Metastatic Prostate
Carcinoma to the Foot with Magnetic Resonance Imaging and Pathologic
Correlation. Foot Ankle Int. 1998; 19(9): 594-597.
16. Uharček P, Mlynček M, Ravinger J. Endometrial Adenocarcinoma
Presenting with an Osseous Metastasis. Gynecol Obstet Invest 2006; 61: 200-202.
17. Desmanet E, Amrani M, Fievez R, Six C. Les Acrometastases. Ann Chir Main Memb 1991; 10(2): 154-157.
18. Cooper JK, Wang F, Swenerton KD. Endometrial adenocarcinoma presenting as
an isolated calcaneal metastasis. Cancer 1994; 73: 2779-2781.
19. Batson OV. The Function of the Vertebral Veins and their Role in the Spread of
Metastases. Ann Surg 1940; 112 : 128-149.
20. Wu K. Bronchgenic carcinoma with metastasis to the foot. A report of two cases.
J Foot Ankle Surg 1995; 34: 322-326.
21. Kricun, ME. Imaging of bone Tumors. Philadelphia, W.B. Saunders, 1993. In: 13.
Schwartz ED, Donahue FI, Bromson MS, Blaise JF. Metastatic Prostate
Carcinoma to the Foot with Magnetic Resonance Imaging and Pathologic
Correlation. Foot Ankle Int. 1998; 19(9): 594-597.
22. Resnick D. Osteomyelitis, septic arthritis, and soft tissue infection on:
mechanisms and situations. In Bone and Joint Imaging, ed. 2, WB Saunders,
Philadelphia, 1996: pp 649-673.
23. Kerin R. The Hand in Metastatic Disease. J Hand Surg. 1987; 12A: 77-83.
24. Sebag-Montefiore DJ, Lam KS, Arnott SJ. Tarsal metastases in a patient with
Rectal Cancer. Br J Rad 1997; 70: 862-864.
25. Hattrup SJ, Amadio PC, Sim FH, Lombardi RM. Metastatic tumours of the
foot and ankle. Foot Ankle 1988; 8: 243-247.